Natália Ransolin
Natália Ransolin
Healthcare facilities allow for a wide range of services performed by different users (e.g., managers, frontline workers, patients, and family members), which demands different solutions from the built environment in terms of components, utilities, and spaces. A large portion of users´ needs arises from interactions between the built environment and the activities carried out by users, such as patient flows and care procedures among and within healthcare units. Finally, EBD should consider integrating design processes with practical approaches more aligned with the complex nature of healthcare services. The insights derived from the system´s modeling can shed light on resilience performance, variability in work conditions, and other factors influencing value generation through the built environment design. The moderator role played by caregivers when dealing with built environment noncompliance must inform lean design solutions supportive of the resilience performance for end-users. In addition, it is worth noting that EBD literature must recognize the inherent variability in healthcare complex environments, assuming that a one-size-fits-all design solution is elusive.
[1] Zhang, Y., Tzortzopoulos, P & Kagioglou, M. (2017). “How evidence-based design supports better value generation for end-users.” In: Proceedings of the 25th Annual Conference of the International Group for Lean Construction, 9th-12th July 2017, Heraklion, Greece. v.1. p. 579-586.
Healthcare environments support both the functional and emotional needs of users. In practice, these can be translated into the avoidance of medical errors, efficiency, or patient comfort. The field of Evidence-based Design (EBD) is concerned with the promotion of healing and fit-for-purpose healthcare services through the built environment. The central idea of EBD is to gather evidence of design solutions that support the achievement of health outcomes [1]. Lighting, external views, temperature, noise, smells, levels of visibility, layout configuration, space for equipment, and accommodation of family members may affect patient healing.
Consistent with a core principle of lean construction, the built environment must envision value generation, and patient requirements should be prioritized in healthcare design. Safety and well-being are goals for addressing patient needs in healthcare services. However, in a dynamic and complex system, defining and achieving value is challenging as it involves conflicting requirements, and some trade offs between safety and well-being, and service requirements need to be considered. For instance, an Intensive Care Unit (ICU) setting with high levels of transparency for patient beds is important from the viewpoint of frontline workers in order to increase patient safety. Meanwhile, transparency can rather hamper patient privacy and comfort, compromising the well-being of patients and family members.
The interdependency among a large number of system elements – activities, users, furniture, equipment, organizational and external factors result in systems with a high degree of complexity: several interactions and variability in meeting a patient's requirements and work conditions can give rise to unexpected events. Hence, healthcare environments could be physically and psychologically stressful for patients, their next-of-kin, and clinical staff.
Dealing with this variability involves frequent adaptations of built environment configurations in order to meet patients´ needs. In practice, healthcare staff plays a key role in moderating the variability in patient safety and well-being. Healthcare workers display mechanisms to avoid variability propagation originated by the built environment failures in fulfilling patient´s requirements. This capability can be understood as a resilient performance, which needs to be investigated in order to support future EBD interventions.
For this purpose, the exploration of activities performed by clinical staff is crucial when designing healthcare environments. In particular, activities closely related to patient safety and well-being must be investigated, as these can trigger a resilience response from workers. Under these circumstances, practical approaches aligned to the complexity of healthcare services are needed to support a more fit-for-purpose built environment design. The Functional Resonance Analysis Method (FRAM) is a useful alternative for processes modeling, shedding light on the system´s interactions and potentially unveiling the resilience displayed by workers[2].
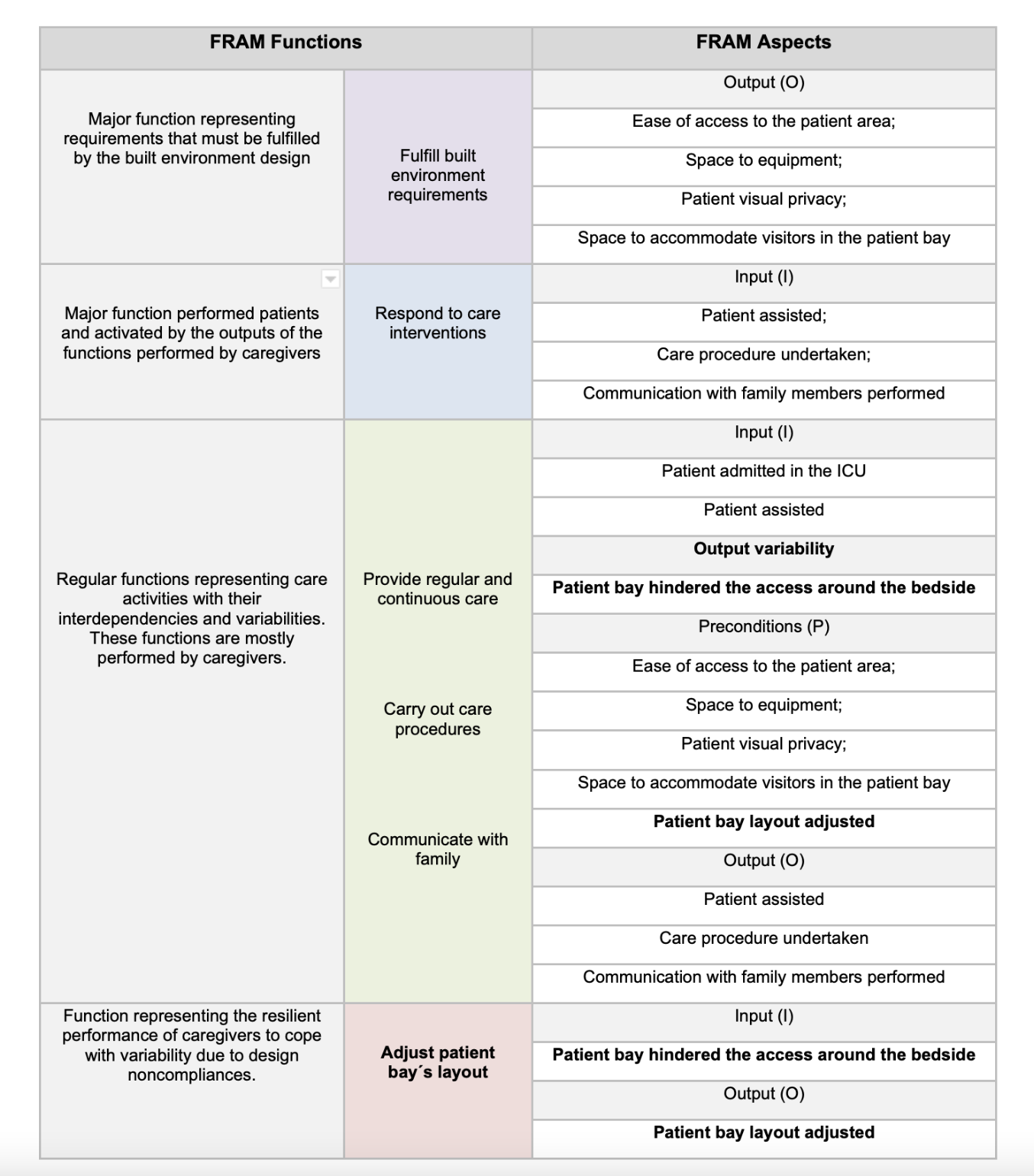
FRAM was applied during an empirical study in an ICU [3]*, resulting in models uncovering how the resilience performance of frontline workers moderate the impact of built environment non compliances to support patient safety and well-being. FRAM functions represent activities performed mainly by agents (e.g., caregivers and patients), and interdependencies are explicit by the connection of their aspects (i.e., input, output, resources, preconditions, time, control). Input and output are the core aspects: while the input starts a function, the output delivers an outcome. In the study, precondition aspects of functions were interpreted as requirements for patient safety and well-being. The built environment noncompliance with these requirements can cause variabilities in functions´ outputs that propagate across the healthcare services.
The figure and the table below illustrate a situation where resilience performance is displayed by the function 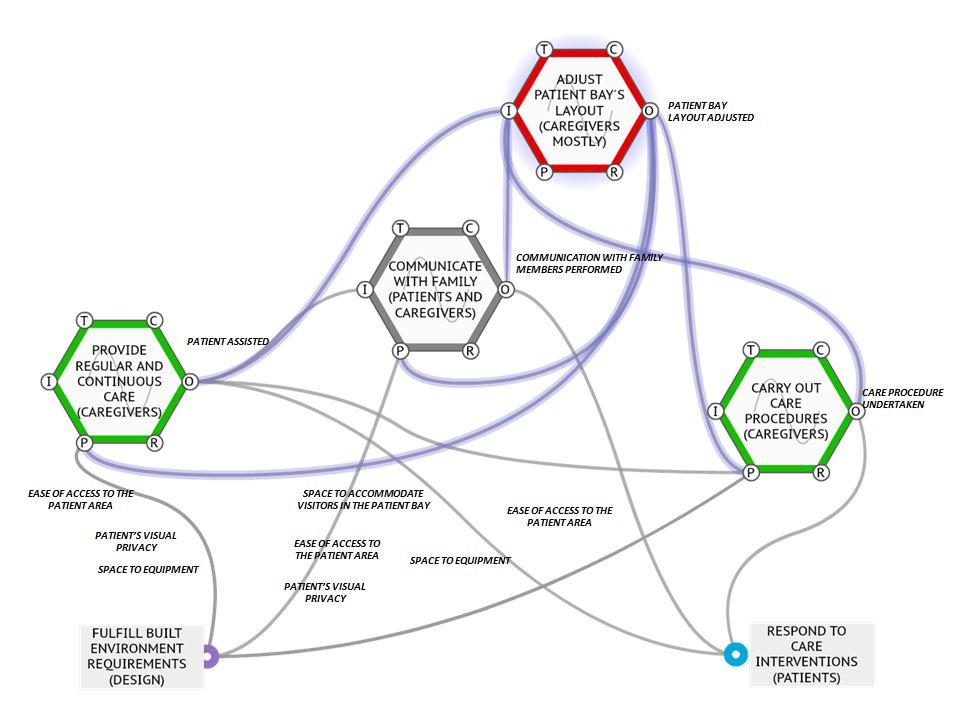
References
[2] Hollnagel, E. (2012). FRAM: the Functional Resonance Analysis Method: Modeling complex socio-technical systems. Ashgate, Burlington.
[3]Ransolin, N., Saurin, T.A.;Formoso, C.T. (2020)b.“Influence of the Built Environment on Patient Safety and Well-being: a Functional Perspective.” In: Tommelein, I.D. and Daniel, E. (eds.). Proc. 28th Annual Conference of the International Group for Lean Construction (IGLC28), Berkeley, California, USA.